Why Infant and Child Circumcision is Not Just a Cosmetic Procedure
As a GP providing infant and child circumcision services on the Gold Coast, I’m often asked whether circumcision is “just cosmetic.” The evidence shows that while circumcision does change the appearance of the penis, it is far more than a purely cosmetic procedure. Modern research, and major policy statements, recognise circumcision as a preventive health measure that can reduce the risk of several medical conditions over a lifetime, particularly when performed in infancy.
For families in the Gold Coast region, the decision usually combines cultural or religious beliefs with clear medical benefits and practical considerations such as access to trained providers and safe, low‑risk techniques.
Why Circumcision Is Not “Just Cosmetic”
Circumcision is the surgical removal of the foreskin (prepuce) that covers the glans of the penis. It has been practised for thousands of years for cultural and religious reasons, but over recent decades the procedure has been closely studied in clinical trials and systematic reviews.
Major evidence reviews and professional bodies now emphasise that:
Circumcision has meaningful medical benefits that outweigh the risks when performed by trained providers with proper pain relief and sterile technique, especially in infancy.
It can prevent or substantially reduce the risk of specific infections and conditions, rather than simply altering appearance.
From a clinical perspective, circumcision sits alongside vaccines and other preventive interventions: elective but supported by data showing reduced disease burden over time.
Evidence‑Based Medical Benefits
1. Lower risk of urinary tract infections in infancy
Urinary tract infections (UTIs) in male infants are more common in boys who are uncircumcised, due in part to bacterial colonisation under the foreskin. Large studies and reviews have shown that circumcised infants have a several‑fold lower risk of UTIs in the first year of life, which also lowers the risk of kidney involvement and hospital admission.
2. Reduced risk of foreskin and penile problems
Circumcision markedly reduces, and often eliminates, conditions related to the foreskin, including:
Phimosis (non‑retractable foreskin causing pain or hygiene issues).
Balanitis and balanoposthitis (inflammation or infection of the glans and foreskin).
Around 10% of males who are not circumcised at birth will later need circumcision for medical reasons. Performing the procedure electively in infancy is generally simpler, safer, and associated with less discomfort and fewer complications than circumcision in older children or adults.
3. Lower lifetime risk of certain sexually transmitted infections
Randomised controlled trials in Africa and supporting epidemiological data show that male circumcision reduces:
Heterosexual acquisition of HIV by about 50–60% in high‑prevalence settings.
Risk of other STIs such as genital ulcer disease, syphilis, herpes simplex virus type 2, and infection with human papillomavirus (HPV).
These data underpinned WHO and UNAIDS recommendations for voluntary medical male circumcision as part of HIV prevention strategies in high‑risk regions. While Australia has lower HIV prevalence, the biological mechanisms (reduced foreskin surface susceptible to microtears and viral entry and altered local microbiome) are relevant to sexual health more broadly.
4. Reduced risk of cancer - penile cancer and partner cervical cancer
Penile cancer is rare but strongly associated with chronic HPV infection and foreskin disease. Evidence synthesised in major reviews shows that circumcision lowers the risk of penile cancer over a lifetime, and may reduce the risk of cervical cancer in female partners by lowering transmission of high‑risk HPV strains.
5. No evidence of harm to sexual function
High‑quality studies assessing adult men after circumcision consistently show no negative impact on sexual function or satisfaction. Many men report unchanged or improved sexual comfort, particularly if they previously had painful foreskin conditions or recurrent infections.
Australian Data: Circumcision as Preventive Health
A recent evidence‑based circumcision policy analysis for Australia sought to quantify how many adverse medical conditions early circumcision can prevent. Using Australian epidemiological data, the authors concluded that:
Early circumcision in boys prevents a substantial number of UTIs, foreskin pathologies, and some STI‑related conditions over the population.
The overall benefits outweigh the risks when the procedure is carried out in a medical setting by trained practitioners.
Global estimates suggest that approximately 25% of men are circumcised worldwide for religious, cultural, medical, or parental choice reasons. This reinforces that circumcision is widely accepted and often chosen with a preventive health rationale, not solely for cosmetic reasons.
Why Gold Coast Families Choose Circumcision
From day‑to‑day clinical experience, supported by the literature, families in the Gold Coast region typically consider circumcision for a mix of reasons:
Preventive health benefits
Parents value the reduced risk of UTIs, foreskin problems, and some STIs, particularly when they have a family history of urological issues or live in communities where circumcision is common.Religious and cultural traditions
Circumcision is an important rite in many faiths and cultures, and families may wish to honour these traditions while ensuring the procedure is done in a modern, sterile medical environment.Future medical convenience
Some parents prefer a one‑time early procedure over the possibility of later surgery for phimosis or recurrent infections, which can be more distressing for older children.Hygiene and practical considerations
The reduced need for foreskin care and easier genital hygiene can be appealing, especially in settings where recurrent balanitis or smegma‑related irritation is common.
As a Gold Coast circumcision GP, my role is not to tell families what to do, but to provide balanced, evidence‑based information and to ensure that if they choose infant or child circumcision, it is performed safely, comfortably, and compassionately.
Safety, Technique and Pain Management
Circumcision has a low complication rate when performed by trained practitioners in a sterile setting, with appropriate anaesthesia and follow‑up. Serious complications are rare, and most minor issues (such as small bleeding or local irritation) are easily managed.
Best‑practice recommendations include:
Use of local anaesthetic and comfort measures for infants and children to minimise pain.
Clear pre‑procedure counselling and written consent covering risks, benefits and aftercare.
Structured follow‑up to assess healing and address any parental concerns.
These standards are what families should expect when seeking circumcision services on the Gold Coast.
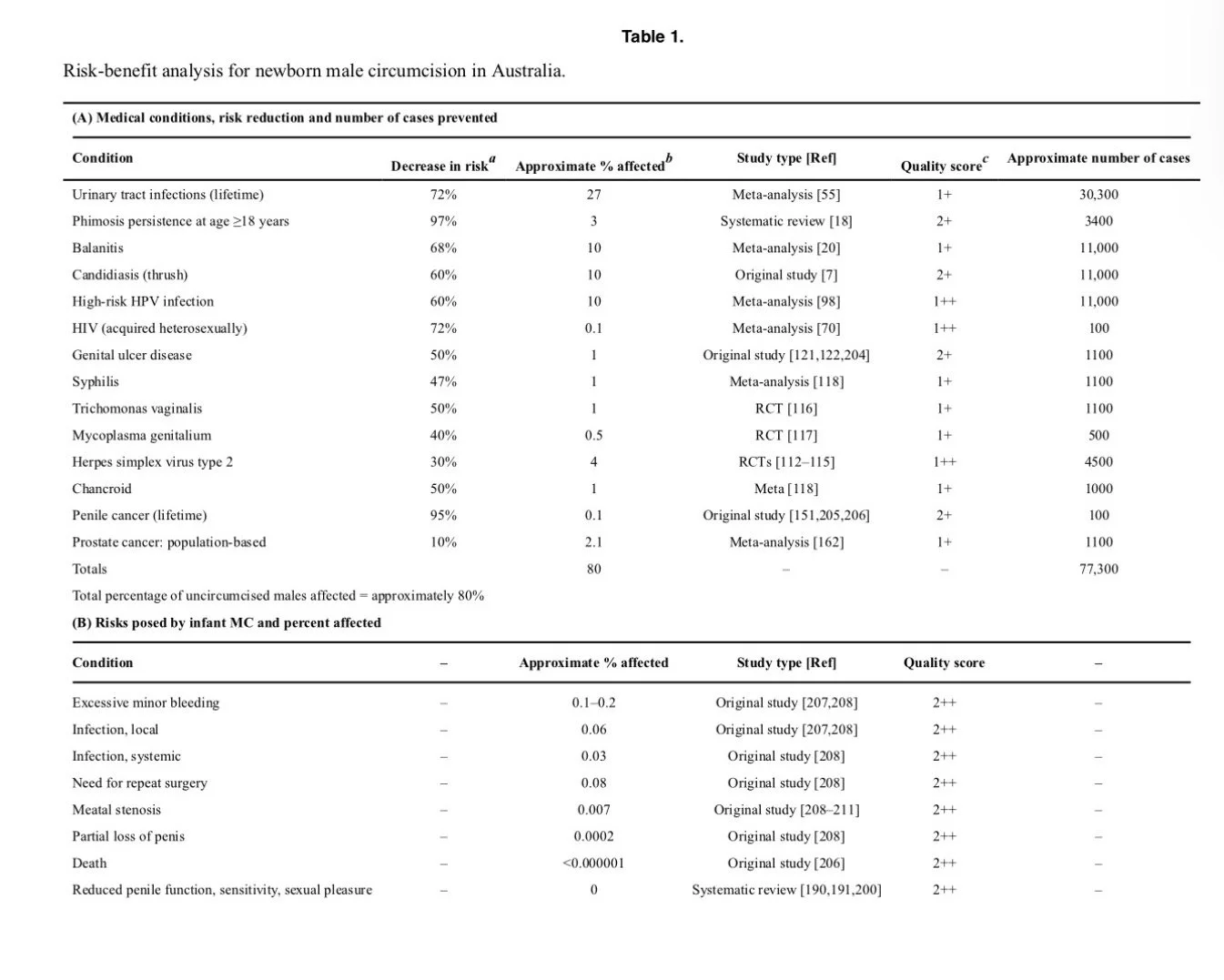
Table 1: From The Journal of Mens Health. 2022;18(6):132.
Reference list
American Academy of Pediatrics Task Force on Circumcision. Male circumcision policy statement. Pediatrics. 2012;130(3):585‑586.
Bossio JA, Pukall CF, Steele SS. Examining penile sensitivity in men following circumcision: a systematic review. J Sex Med. 2016;13(5):777‑787.
Centers for Disease Control and Prevention. Background, methods, and synthesis of scientific information used to inform “Information for providers to share with male patients”. CDC; 2018.
El Bcheraoui C, et al. Safety and efficacy of non‑therapeutic male circumcision: a systematic review. J Urol. 2011;185(5):1494‑1500.
Grund JM, Bryant TS, Jackson I, et al. Association between male circumcision and women’s biomedical health outcomes: a systematic review. Lancet Glob Health. 2017;5(11):e1113‑e1122.
Grund JM, et al. Early infant male circumcision: systematic review, risk‑benefit, and policy implications for Australia and New Zealand. Arch Dis Child. 2017;102(8):694‑700.
Kacker S, Tobian AAR, Reed JB, et al. Costs and cost‑effectiveness of adult male circumcision for HIV prevention in men in a high HIV prevalence setting. J Acquir Immune Defic Syndr. 2013;64(4):e125‑e134.pubmed.
Larke NL, Thomas SL, Silva LM, Weiss HA. Male circumcision and penile cancer: a systematic review. BMC Cancer. 2011;11:278.
Lotti F, et al. Pros and cons of circumcision: an evidence‑based overview. Clin Microbiol Infect. 2016;22(10):851‑857.
Marcell AV. Greater benefits of infant circumcision. Johns Hopkins Medicine. 2012.
Mazen AI. Non‑therapeutic infant male circumcision: evidence, ethics, and international law perspectives. Saudi Med J. 2016;37(9):941‑947.
Morris BJ, Bailis SA, Wiswell TE. Circumcision rates in Australia: evidence‑based policy and practice. Open J Prev Med. 2012;2(3):304‑315.
Morris BJ, Cooper DA, Wodak AD, et al. Evidence‑based circumcision policy for Australia. World J Clin Urol. 2013;2(3):89‑102.
Morris BJ, et al. CDC’s male circumcision recommendations represent a key public health measure. Int J Child Health Hum Dev. 2017;10(1):69‑79.
Morris BJ, Katelaris A, Blumenthal NJ, Hajoona M, Sheen AC, Schrieber L, Lumbers ER, Wodak AD, Katelaris P. Evidence‑based circumcision policy for Australia. J Mens Health. 2022;18(6):132.
Morris BJ, Krieger JN. Male circumcision: assessment of health benefits and risks. Sex Med. 2013;1(2):109‑120.
Morris BJ, Waskett JH, Gray RH. The medical benefits of male circumcision. J Sex Med. 2012;9(2):577‑592.
Morris BJ, Wiswell TE. Circumcision and lifetime risk of urinary tract infection. J Urol. 2013;189(6):2118‑2124.
Morris BJ, et al. CDC’s male circumcision recommendations represent a key public health measure. Int J Child Health Hum Dev. 2017;10(1):69‑79.
Tobian AAR, Kacker S, Quinn TC. The effect of male circumcision on HIV transmission and acquisition. Curr HIV Res. 2014;12(4):197‑205.
Weiss HA, Larke NL, Halperin D, Schenker I. Complications of circumcision in male neonates, infants and children: a systematic review. BMC Urol. 2010;10:2.
Waskett JH, Morris BJ. Re: The medical evidence on non‑therapeutic circumcision of infants and boys-setting the record straight. Int J Impot Res. 2022;34(5):490‑492.
World Health Organization, UNAIDS. New data on male circumcision and HIV prevention: policy and programme implications. WHO; 2007.