Oral Ties Explained: Types, Symptoms and Why Early Release Matters”
As a GP specialising in oral tie releases, I often encounter questions about the various types of oral ties, what they are, what they look like, where they are and their impact. Understanding these can help parents seek timely treatment. Below you will find a very brief summary of the types of oral ties.
The Different Types of Oral Ties
1.Tongue Ties (Ankyloglossia)
Tongue tie occurs when the lingual frenulum - the tissue connecting the underside of the tongue to the floor of the mouth - is unusually short or tight, restricting tongue movement.
The classification varies depending on your source, but the commonly used Coryllos classification separates tongue ties into 4 types.
This classification helps in diagnosing and determining the severity of tongue-tie conditions, but it doesn’t reflect the severity of the symptoms. As such, a functional assessment is always necessary to complete the diagnosis.
Types 1 & 2 are considered the “classical” type of tongue ties but type 3 and 4 can cause just as significant symptoms but are commonly missed.

Table 1.1 – The Coryllos Classification of tongue ties
2. Lip Ties (maxillary labial frenulum attachments)
The labial frenulum connects the upper lip to the gum. When tight or thick, it can restrict lip movement, potentially causing breastfeeding difficulties, poor latch, or dental hygiene challenges.
The Kotlow lip tie classification is a widely used system for describing the severity and location of upper lip ties in infants and children. It is based on where the frenulum attaches to the gingival (gum) tissue, helping clinicians assess the potential impact on function.
Class I is rarely restrictive, Class II and III may affect feeding or oral hygiene, depending on tightness, while class IV is most restrictive and most likely to cause functional problems. However, although the classification system helps guide treatment decisions, it does not always indicate symptom severity, as some children may compensate well despite a higher class tie.

Table 2.1 The Kotlow lip tie classification
3. Cheek Ties (Buccal Ties)
Less common, buccal ties involve a mucosal attachment from the cheek to the gum, which may affect oral function and comfort. They are classified based on the membrane attachment site.
Class 1 – Mucosal Attachment
Class 2 – Gingival Attachment
Class 3 – Alveolar Ridge Attachment
Under normal circumstances, the buccal frenulum supports the structure of the cheeks and lips. The membrane extends to both sides of your mouth, but if it’s too tight, it has been said to restrict normal cheek movement, interfering with the feeding process.
Why Early Diagnosis and Treatment Matter
Oral ties can interfere with breastfeeding, speech development, dental health, and even posture or breathing. Early assessment by a trained professional ensures appropriate management - whether it is monitoring, feeding support, bodywork, frenotomy, or frenuloplasty - leading to better outcomes.
If you have concerns, I am happy to consult with you and your family to discuss the symptoms and help make a proper assessment and diagnosis. To arrange an appointment, please call Medical on Robina to discuss your concerns with me.
References
Messner, A. H., Lalakea, M. L., Aby, J., Macmahon, J., & Meara, J. G. (2000). Ankyloglossia: incidence and associated feeding difficulties. Archives of Otolaryngology–Head & Neck Surgery, 126(1), 36-39. https://doi.org/10.1001/archotol.126.1.36
Hogan, M., Westcott, C., & Griffiths, M. (2005). Tongue-tie and frenotomy in infants with breastfeeding problems: A prospective, randomized trial. Pediatrics, 116(3), e1–e7. Randomized, controlled trial of division of tongue‐tie in infants with feeding problems - Hogan - 2005 - Journal of Paediatrics and Child Health - Wiley Online Library
Geddes, D. T., Langton, D. B., Gollow, I., Jacobs, L. A., Hartmann, P. E., & Simmer, K. (2008). Frenulotomy for breastfeeding infants with ankyloglossia: effect on milk removal and sucking mechanism as imaged by ultrasound. Pediatrics, 122(1), e188-e194. https://doi.org/10.1542/peds.2007-2087
American Academy of Pediatrics. (2012). Clinical Report: Ankyloglossia (Tongue-tie) and Breastfeeding. Pediatrics, 129(6), e1572-e1578. https://doi.org/10.1542/peds.2011-3552
If you suspect an oral tie is affecting feeding or speech, consult a healthcare professional experienced in diagnosis and release procedures for personalised care.Srinivasan, A., Al Khoury, A., Puzhko, S., Dobrich, C., Stern, M., Mitnick, H., & Goldfarb, L. (2019). Frenotomy in infants with tongue-tie and breastfeeding problems. Journal of Human Lactation, 35(4), 706–712. https://doi.org/10.1177/0890334418816973
A GP’s Guide: When Your Son May Need a Circumcision? Understanding The Medical Indications
As a GP specializing in circumcision procedures, I frequently encounter questions about the medical reasons for circumcision or people asking if they should have their son circumcised. This guide outlines the key indications, helping patients and families make informed decisions.
What Is Circumcision?
Circumcision is the surgical removal of the foreskin covering the head of the penis. While often performed for cultural or religious reasons, there are also well-established medical indications.
Medical Indications for Circumcision
Absolute Medical Reasons
Pathological Phimosis
Phimosis is the inability to retract the foreskin. When caused by scarring or chronic inflammation (such as lichen sclerosis or balanitis xerotica obliterans), circumcision may be necessary if topical treatments aren’t adequate.
Signs of pathological phimosis include:
Inability to retract the foreskin (note this can be normal in younger boys)
Ballooning or bulging of the foreskin during urination
Pain or discomfort during urination, erection, or sexual activity
Redness, swelling or soreness of the foreskin
Difficulty urinating where the tight foreskin may block the flow leading to a weak stream or inability to empty the bladder fully
Discharge or odour due
White ring or scar tissue may indicate lichen sclerosis or repeated infections.
If your son is experiencing any of these symptoms, then he may have phimosis and benefit from a circumcision.

Figure 1.1 Symptoms of Phimosis
Recurrent Balanitis or Balanoposthitis
Repeated infections or inflammation of the glans (balanitis) or foreskin (balanoposthitis) can be indications for circumcision if other treatments fail or if they are recurrent and impacting life.
Relative Medical Reasons
Recurrent Urinary Tract Infections (UTIs)
In boys with recurrent UTIs, especially those with underlying urological abnormalities, circumcision may be considered, and the latter case is often recommended.
Paraphimosis
This is an emergency where the retracted foreskin cannot be returned to its normal position. Circumcision may be needed if episodes recur or if reduction is unsuccessful.

Figure 1.2 Phimosis vs Paraphimosis
Penile or Preputial Neoplasms
Suspicious or cancerous lesions may require circumcision for diagnosis or treatment.
Prevention of Sexually Transmitted Infections (STIs)
There is evidence that circumcision reduces the risk of HIV transmission in high-prevalence areas, as well as HPV rates though the benefit is less clear in low-prevalence regions.
Non-Medical Reasons
Many circumcisions are also performed for cultural, religious, or personal reasons.
As a medical practitioner, it is important to ensure that parents or patients are fully informed about the risks and benefits, especially when the procedure is not medically indicated.
Why Choose a GP Specializing in Circumcision?
As a General Practitioner with specialized training and experience in circumcision procedures, I am dedicated to providing safe, evidence-based care. I ensure that all patients and families receive thorough information, appropriate pain management, and high-quality follow-up. Circumcision is a decision that should be made carefully, with a full discussion of the risks, benefits, and available alternatives.
Where circumcision is considered the best option, I offer the plastibell technique for boys up to 12 or 13 years of age (depending on their size). The procedure is performed in my consulting rooms, eliminating the need for anaesthesia, costly hospital fees, or lengthy waitlists.
If you are considering circumcision for your son, if you think your son requires a circumcision, or if your older son is requesting the procedure, I am happy to consult with you and your family to discuss the process, risks, benefits, and necessity. To arrange an appointment, please call Medical on Robina.

Table 1.1 Reasons for Circumcision Summary
Reference List
· USANZ Guidelines: How to Perform Circumcision on Infant Males. Available at: USANZ - Guidelines on how to Perform Circumcision on Infant Males
· NHS: Circumcision in Men – Medical Reasons. Available at: Circumcision in men - NHS
· USANZ: Quality and Safety Considerations. Available at: USANZ - Guidelines on how to Perform Circumcision on Infant Males
· Patient.info: Indications for Circumcision. Available at: Circumcision: Assessment and Complications | Doctor
· The Urology Place: Adult Circumcision Before and After Photos. Available at: San Antonio Urology | Board Certified | Experienced Doctors
· Wikimedia Commons: Circumcision Images. Available at: Category:Circumcision - Wikimedia Commons
· Medical aspects of male circumcision. BMJ. 2007 Dec 8;335 (7631): 1206 – 1209. Morris BJ, Wiswell TE. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC2128632/1
· Circumcision StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.Stang HJ, Snellman LW. Available at: https://www.ncbi.nlm.nih.gov/books/NBK535436/2
· Male circumcision: Global Trends and Determinants of Prevalence, Safety and Acceptability. World Health Organization. 2007. Available at: https://apps.who.int?iris/bitstream/handle/10665/43749/9789241596169_eng.pdf
· Adult Circumcision. American Family Physician.1999 Mar 15;59(6):1514-1518. Weiss HA, Larke N, Halperin D, Schenker I. Available at: https://www.aafp.org/pubs/afp/issues/1999/0315/p1514.html
· Circumcision for phimosis and other medical indications in Western Australian boys. Med J Aust. 2003 Feb 17;178(4):155-8. Spilsbury K, Semmens JB, Wisniewski ZS, Holman CD. Available at: https://www.mja.com.au/system/files/issues/178_04_170203/spi10278_fm.pdf
· Circumcision. Raising Children Network. October 2024. Available at: https://raisingchildren.net.au/guides/a-z-health-reference/circumcsion
· Circumcision Clinical Presentation: Physical Examination. Medscape. Updated: Jan 31, 2020. Available at: https://emedicine.medscape.com/article/1015820-clinical
· Circumcision of Infant Males. Royal Australasian College of Physicians (RACP). Position Statement. 2010. Available at: racp-circumcision-of-infant-males-position-statement.pdf
Circumcision in Infants and Children: Weighing The Benefits and Risks
As a Gold Coast GP specialising in circumcision and tongue-tie releases, I’m often asked by parents about the benefits and risks of infant circumcision. With so much information, and misinformation, online - it’s essential to base decisions on the best available medical evidence and guidelines. Here’s what you need to know if you’re considering circumcision or tongue tie procedures for your child.
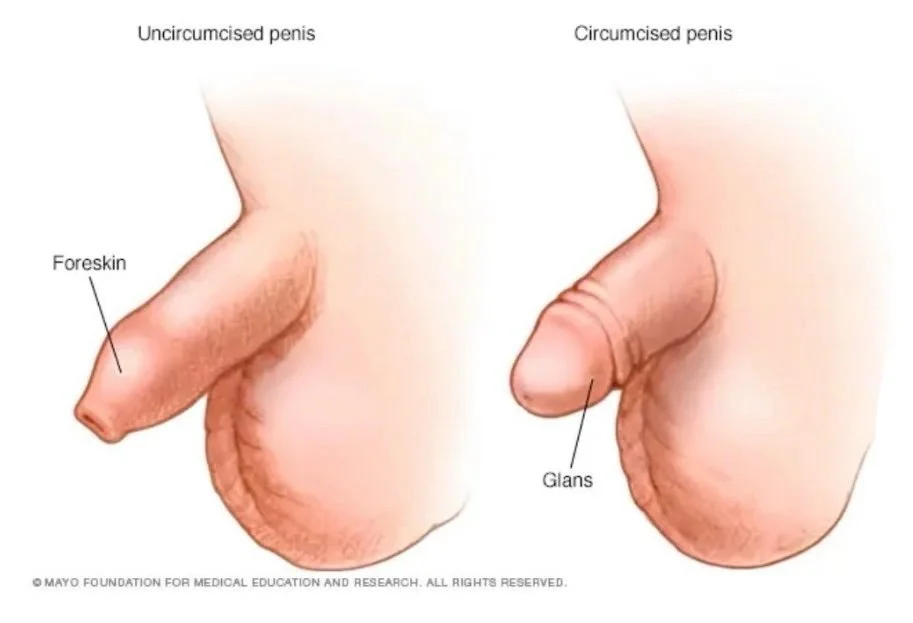
A circumcision is a surgical procedure that involves the removal of the foreskin, which is the fold of skin covering the tip (glans) of the penis. This procedure is often performed for medical, cultural, religious or personal reasons. In infants and children, circumcision is typically done under local anaesthesia by a trained medical professional in a sterile environment to minimise risks.
Figure 1: The Penis before and after circumcision
Circumcision in Infants and Children: What are the Benefits?
Reduced Risk of Infections
Urinary Tract Infections (UTIs): Circumcision lowers the risk of UTIs in infants, especially those with urinary tract or kidney abnormalities. The Association of American Physicians (AAP) reported that circumcised infants have a 10x lower risk of urinary tract infections in their first year.
Sexually Transmitted Infections (STIs): There is evidence that circumcised males have a reduced risk of acquiring HIV and certain other STIs, including HPV and herpes simplex virus. Some studies have shown a 50 -60% lower risk of HIV and HPV transmission in adulthood. However, these benefits are most relevant in regions with high STI prevalence, and this is far less pronounced in Australia.
Reduced Risk of Cancer
Penile Cancer: Circumcision is associated with a slightly lower risk of penile cancer, and the benefit has been shown to be most significant when circumcision is performed in infancy or childhood, before potential exposure to human papillomavirus (HPV) and other risk factors. However, this cancer is extremely rare in Australia and New Zealand, and the absolute reduction in risk is very small.
Prostate Cancer: Some studies suggest that circumcision may be linked to a lower risk of prostate cancer due to reduced risk of sexually transmitted infections that may contribute to prostate inflammation and subsequent cancer risk. However, again, the evidence for a protective effect against prostate cancer is less robust than for penile cancer, and the association is not considered strong enough to recommend circumcision solely for prostate cancer prevention
Prevention of Foreskin-Related Conditions
Circumcision can prevent conditions such as phimosis (tight foreskin), balanitis (inflammation of the glans) and recurrent infections. Over a lifetime, more than half of uncircumcised males may experience a foreskin-related issue.
Easier Hygiene
Removing the foreskin makes penile hygiene simpler, reducing the risk of smegma buildup and infections and irritation.
Risks and Considerations of Circumcision
Surgical Risks
Complications are rare when performed by experienced professionals, but can include bleeding, infection, scarring (1–2% of cases, usually minor), and very rarely, injury to the penis (<0.1% risk).
Pain and Recovery
While the procedure is generally quick, pain management is important.
Topical anaesthesia is used prior to local anaesthesia to minimise discomfort during the procedure
Post operatively, most infants recover within 7–10 days while older boys can take up to 2 weeks and simple analgesia is usually more than adequate.
Ethical and Cultural Considerations
Infant circumcision involves important ethical considerations because it is a non-therapeutic procedure performed on babies who cannot consent, and it permanently removes tissue.
While the procedure is generally safe and may offer some health benefits, as discussed, it also carries risks and raises questions about respecting the child’s future autonomy and bodily integrity.

What do Medical Organisations say?
Most medical organisations agree the health benefits slightly outweigh the risks, but not enough to recommend routine circumcision for all newborns.
The Royal Australasian College of Physicians (RACP) reviewed the current evidence and found that while circumcision is generally safe, the frequency of diseases it can prevent is low in Australia and New Zealand. Therefore, the RACP does not recommend routine infant circumcision for healthy boys, stating that “the benefits do not clearly outweigh the risks”. They acknowledge there are clear benefits in certain circumstances – for instance, for infants with significant urinary tract abnormalities or recurrent infections.
The RACP supports parental choice provided:
The procedure is performed by a qualified, experienced practitioner.
Accurate, unbiased information about risks and benefits is provided.
Appropriate anaesthesia and a child-friendly environment are ensured for safety.
The Urological Society of Australia and New Zealand (USANZ), and other bodies support the RACP statement, emphasising that the risks of non-medical circumcision generally outweigh the benefits for well infants.
Conclusion
Circumcision is a safe and effective procedure with well-documented benefits for certain medical conditions. However, for most healthy infants in Australia, the risks and ethical considerations mean routine circumcision is not universally recommended. The decision is personal - parents should weigh the evidence, consider their values and consult with a trusted, experienced GP.
If you have questions about circumcision or tongue-tie procedures for your infant or child, I am located on the Gold Coast at Medical On Robina and you can book a consultation for expert, compassionate advice.
Circumcision and Tongue Tie Services on the Gold Coast
As a GP with a focus on circumcision and tongue-tie releases, I provide:
Evidence-based advice tailored to your child’s needs and your family’s values.
Safe, gentle procedures using the latest techniques and pain management protocols.
Comprehensive aftercare to ensure the best outcomes for your child.
Frequently Asked Questions
Is circumcision covered by Medicare?
In Australia, circumcision is only covered by Medicare if medically necessary (e.g., for recurrent infections or phimosis).Are there alternatives to circumcision?
Yes - good hygiene, safe sexual practices and regular medical checkups can prevent most foreskin-related issues in uncircumcised boys.What about tongue ties?
Tongue-tie (ankyloglossia) can affect feeding, speech and oral health. If you have concerns about your child’s tongue movement or feeding, an assessment by an experienced provider can determine if a release may be appropriate.
Resources and Further Reading
PubMed. “Pros and cons of circumcision: an evidence-based overview.” Pros and cons of circumcision: an evidence-based overview - PubMed
University of Sydney. (2017, February 8). Male infant circumcision has a 200 to one risk-benefit: research. University of Sydney News. Male infant circumcision has a 200 to one risk-benefit: research - The University of Sydney
Raising Children Network. (n.d.). Circumcision. Retrieved from https://raisingchildren.net.au/guides/a-z-health-reference/circumcision
Moses, S., Bailey, R. C., & Ronald, A. R. (1998). Male circumcision: assessment of health benefits and risks. Sexually Transmitted Infections, 74(5), 368–373. https://doi.org/10.1136/sti.74.5.368
Morris, B. J., Bailis, S. A., & Wiswell, T. E. (2017). Early infant male circumcision: Systematic review, risk-benefit analysis, and progress in policy. World Journal of Clinical Pediatrics, 6(1), 89–102. https://doi.org/10.5409/wjcp.v6.i1.89**
Royal Australasian College of Physicians. (2022). Circumcision of infant males [PDF]. Royal Australasian College of Physicians. https://www.racp.edu.au/docs/default-source/advocacy-library/racp-circumcision-of-infant-males-position-statement.pdf?sfvrsn=92edd11a_4
Urological Society of Australia and New Zealand. (n.d.). Guidelines on how to perform circumcision on infant males. Urological Society of Australia and New Zealand. https://www.usanz.org.au/info-resources/position-statements-guidelines
Urological Society of Australia and New Zealand. (n.d.). RACP position statement on circumcision of infant males. Urological Society of Australia and New Zealand. https://www.usanz.org.au/info-resources/position-statements-guidelines
Nature. (n.d.). Royal Australasian College of Physicians' recent policy on infant circumcision. Nature. https://www.nature.com/articles/s41390-024-03190-8.pdf
Pediatric Research. “Detrimental to public health: Royal Australasian College of Physicians’ recent policy on infant circumcision.” https://www.nature.com/articles/s41390-024-03190-8.pdf
RACP. Circumcision – Parent information. circumcision-brochure-2024.pdf
RACP. Policy and Advocacy Library. https://www.racp.edu.au/policy-and-advocacy/search#:~:text=The%20RACP%20submission%20refers%20to%20specific%20proposals%20for,Policy%20and%20Advocacy%20Library%20for%20published%20policy%20documents.
World Journal of Clinical Pediatrics. “Early infant male circumcision: Systematic
Mayo Foundation for Medical Education and Research. (2024). Circumcision: What you can expect. Mayo Clinic. https://www.mayoclinic.org/tests-procedures/circumcision/about/pac-20393550
Keywords: Circumcision Gold Coast, Infant circumcision, Child circumcision, Paediatric circumcision, Circumcision risks, Circumcision benefits, RACP circumcision guidelines, Circumcision clinic Gold Coast, Tongue tie Gold Coast, Tongue tie release,
Understanding Tongue Tie (Ankyloglossia): A Comprehensive Guide for Parents and Healthcare Professionals
Tongue tie, medically known as ankyloglossia, is a condition that has generated significant discussion in both clinical and parenting circles. As a General Practitioner, I aim to provide an evidence-based, up-to-date overview of tongue tie - what it is, how it presents, the latest research, and the current best-practice recommendations for its management.
Tongue tie occurs when the thin band of tissue connecting the underside of the tongue to the floor of the mouth (the lingual frenulum) is unusually short, thick, or tight. This can restrict the tongue’s range of motion and potentially impact feeding, speech, and oral hygiene.
Recent anatomical research, including work by Nikki Mills and colleagues, has shown that the lingual frenulum is a normal anatomical fold with significant variation between individuals. Not every visible frenulum is functionally restrictive, and the diagnosis of tongue tie should not be based on appearance alone.
Symptoms and Signs of Tongue Tie
Tongue tie can present with a spectrum of symptoms, most commonly in infants who are breastfeeding. Key symptoms and signs include:
Breastfeeding difficulties: Poor latch, prolonged feeds, poor milk transfer, clicking sounds, or the infant slipping off the breast, frustrated feeds, and frequent feeds.
Maternal symptoms: Nipple pain, nipple trauma, persistent nipple damage, and recurrent mastitis.
Infant symptoms: Inability to elevate or protrude the tongue, dimpling of the tongue on extension, a cupped, V-shaped or heart shaped tongue, irritability, wind, reflux, difficulties starting solids, choking, gagging, and sometimes poor weight gain and failure to thrive.
Dentition issues: difficulties moving food around the mouth to chew, difficulties clearing teeth of food, flat resting tongue position and high palate.
Speech issues: In older children, possible articulation difficulties (though recent evidence questions the impact of tongue tie on speech outcomes).
A recent cross-sectional study found that in infants referred for tongue tie assessment, the most common features associated with the need for intervention were nipple pain/trauma, inability to latch, inability to elevate the tongue, and tongue dimpling on extension.
How Is Tongue Tie Diagnosed?
Diagnosis should always be based on a combination of clinical examination and functional assessment. Major guidelines and best-practice recommendations emphasize:
Assessment of tongue movement and function: Not just the appearance of the frenulum.
Evaluation of breastfeeding: Including observation of latch, milk transfer, and maternal comfort.
Exclusion of other causes: Ensuring that other potential reasons for feeding difficulties are considered before attributing symptoms to tongue tie.
Tools such as the Hazelbaker Assessment Tool for Lingual Frenulum Function (HATLFF) are sometimes used to standardize assessment.
Current Evidence: What Does the Latest Research Say?
Breastfeeding and Tongue Tie
Ultrasound studies have shown that effective milk transfer is more dependent on the intra-oral vacuum created by the baby’s jaw and tongue, rather than just tongue movement. Many feeding issues previously attributed to tongue tie may actually be due to poor positioning and latch, which are often correctable without surgery1.
Surgical release (frenotomy) has shown to improve breast feeding effectiveness, reduce nipple pian, increase maternal self-efficacy and reduce gastro-oesophageal reflux disease.
Treatment Options for Tongue Tie

Conservative (Non-Surgical) Management
First-line approach: For most infants, non-surgical strategies are recommended initially. These include:
Optimizing breastfeeding technique (positioning and latch)
Lactation consultant support
Speech pathology support
Bodywork with an orofacial myologist, osteopath, chiropractor, or paediatric physiotherapist
Addressing milk supply issues with pumping or medications such as motilium.
Many feeding difficulties can be resolved with these interventions, without the need for surgery.
Surgical Management: Frenotomy
Indication: Frenotomy should only be considered when there is a clearly defined structural restriction causing persistent functional feeding difficulty, and when conservative measures have failed.
Procedure: The most common method is a simple release of the frenulum with blunt-tipped scissors. Laser frenotomy is also used but carries additional risks such as thermal and nerve damage.
Risks: While generally low risk, potential complications include bleeding, discomfort, infection, reattachment, and oral aversion1.
Post-Operative Care
Immediate breastfeeding support is recommended after the procedure to maximize the chances of successful feeding and minimize complications15.
Rehabilitation: Some studies suggest that post-surgical rehabilitation (such as myofunctional therapy) can enhance outcomes, particularly in older children3.
Best-Practice Recommendations
Based on the latest evidence and guidelines from organizations such as the Academy of Breastfeeding Medicine, Speech Pathology Australia, and the Australian Dental Association, the following approach is recommended:
Assess function, not just appearance.
Try conservative management first.
Reserve surgery for clear, persistent functional problems.
Use scissors rather than laser for infants.
Provide comprehensive breastfeeding support post-procedure.
Avoid unnecessary release of lip or cheek ties.
Key Takeaways for Parents and Healthcare Professionals
Tongue tie is common, but not all cases require intervention.
Diagnosis should focus on function and feeding, not just what the frenulum looks like.
Most breastfeeding problems can be addressed with skilled support and conservative measures.
Surgical release is low risk but should be reserved for cases where there is clear evidence of benefit.
Recent References and Further Reading
· Douglas, P., & Geddes, D. (2018). Ultrasound imaging of tongue function in breastfeeding. Midwifery, 62, 1–8
· Mills, N., Pransky, S. M., Geddes, D. T., & Mirjalili, S. A. (2019). Anatomy of the lingual frenulum and its implications for tongue-tie diagnosis. Clinical Anatomy, 32(7), 1025–1032
· Melong, C., Smith, A., & Johnson, L. (2024). Speech outcomes following tongue-tie (ankyloglossia) release in children: A prospective study. International Journal of Pediatric Otorhinolaryngology, 174, 111234
· Ferrés-Amat, E., Pastor-Vera, T., Rodriguez-Alessi, P., Ferrés-Amat, E., Mareque-Bueno, S., & Ferrés-Padró, E. (2022). Outcomes of tongue-tie release and myofunctional therapy: A systematic review. Journal of Clinical Medicine, 11(4), 1022.
· S mith, J., Lee, A., & Patel, R. (2024). Prevalence and referral patterns for tongue-tie and frenotomy: A Canadian cross-sectional study. Canadian Journal of Paediatrics, 29(2), 85–92
· Royal Hospital for Women (NSW Health). (2019, reviewed 2024). Tongue Tie Assesment and Management Guidlines. Sydney: NSW Health
· Cordray, H., Raol, N. P., Mahendran, G. N., Tey, C. S., Nemeth, J., Sutcliffe, A., Ingram, J., & Sharp, W. G. (2024). Quantitative impact of frenotomy on breastfeeding: A systematic review and meta-analysis. Pediatric Research, 95(1), 34–42.
· Bruney, T. L., O'Shea, J. E., & Watson, J. (2022). Systematic review of the evidence for resolution of common breastfeeding problems—Ankyloglossia (Tongue Tie). Acta Paediatica, 111(5), 1007–1015.
Conclusion
Tongue tie is a nuanced condition that requires careful assessment and a balanced, evidence-based approach. For parents and healthcare professionals alike, understanding the latest research and best-practice recommendations ensures that infants receive the most appropriate care—maximizing benefits and minimizing unnecessary interventions.
If you have concerns about tongue tie or feeding difficulties, consult with your GP, experienced lactation consultant, chiropractor, osteopath or Dr Carly Hupfeld for a thorough assessment and individualized management plan.
“A tongue-tie diagnosis should never be based on appearance alone—it requires evidence of restricted movement and functional feeding difficulty.”
This blog is intended for educational purposes and does not replace individualized medical advice. For further information or assessment, please consult your healthcare provider.
Book a Consultation with Dr Carly Hupfeld
Whether you're ready to book or just want to learn more, we’re here to help you make the best decision for your family.
Dr Carly Hupfeld assess and manages oral ties and performs circumcisions:
Medical On Robina
T3/299 Scottsdale Dr, Robina QLD 4226
(07) 5690 1290
Understanding Circumcision in Australia: What Families Need to Know?
A Look at the Numbers

For many Australian families, deciding whether to circumcise their son involves balancing medical advice, cultural values, and personal beliefs.
As a GP with a special interest in circumcision, I often get asked: “How common is circumcision in Australia?” The answer is nuanced and understanding the numbers can help parents make informed choices.
How Common Is Circumcision In Australia?
Newborn Circumcision Rates
Today, around 1 in 5 newborn boys in Australia, approximately 20%, undergo circumcision. This marks a significant shift from the mid-20th century when the procedure was far more routine. The decline is largely due to updated medical recommendations and changing social attitudes.
Overall Male Circumcision Rates
Approximately 30% of Australian males have been circumcised, reflecting more common practices in previous generations and ongoing traditions within certain communities.
Where Do These Numbers Come From?
Circumcision data in Australia is sourced from:
Hospital and Medicare Records: Documenting procedures by registered medical professionals.
National Surveys and Studies: These provide broader estimates, though data collection methods vary.
Regional Tracking: Some states and hospitals monitor rates more closely, but there is no national registry.
Why Real Rates May Be Higher Than Reported?
While official statistics provide valuable insights, they may underestimate the true prevalence of circumcision. This is because:
Private Clinic Procedures: Many families choose to have circumcisions performed by private practitioners. These procedures may not be captured in public health records or Medicare databases, especially if families are not eligible for Medicare rebates.
Religious or Community Circumcisions: These are often performed outside traditional medical settings.
Historical Record Gaps: Earlier procedures, especially before the digital era, may not appear in current data.
Circumcision in Australia vs. the World

Globally, around 38% of males are circumcised. However, this varies widely:
In Muslim-majority countries, circumcision is nearly universal (over 99%).
In regions like Western Europe and Latin America, circumcision is less common.
Australia falls in the middle, with decisions driven by personal, cultural, and medical considerations.
In countries with strong religious or cultural traditions, circumcision rates exceed 99% - especially in Muslim-majority nations. In contrast, rates in Western Europe and Latin America are far lower.
Making the Right Choice for Your Child
If you’re exploring circumcision for your son, professional guidance can make all the difference.
As a doctor with extensive experience in newborn and childhood circumcision, I’m here to provide:
Accurate, evidence-based information
Safe, caring, and comfortable procedures
Supportive consultation for families from all backgrounds
Book a Consultation with Dr Carly Hupfeld
Whether you're ready to book or just want to learn more, we’re here to help you make the best decision for your family.
Dr Carly Hupfeld specialises in circumcision and oral ties at:
Medical On Robina
T3/299 Scottsdale Dr, Robina QLD 4226
(07) 5690 1290
ReferencesCircumcision By Country 2025Circumcision | healthdirectCircumcision in Perth for children | Paediatric Surgeons Murdochmapsfacts | The countries with the highest male circumcision rates in the world (countries with a minimum rate of 85% included only) are: . 🇵🇸... | InstagramThe Facts On Circumcision: FAQ’s, What You Need To Know - Circumcision Vasectomy AustraliaKNMG. The non-therapeutic circumcision of male minors. KNMG, May 2010. Available here.