Not Just a Little Tie: When a “Mild” Tongue Tie Isn’t Mild at All
As a tongue tie doctor on the Gold Coast, I often meet families who have been told their baby only has a ‘little tie’ despite ongoing problems. I find parents are often reassured that their baby has “just a little tongue tie,” especially when the frenulum doesn’t appear severe at first glance. However, even a subtle-looking tie can significantly restrict tongue movement, contribute to feeding difficulties, and impact oral function over time.
This raises an important question: what does a “small/little” tongue tie actually mean? Does it refer to the visible length of the frenulum - where a short tie may still cause considerable restriction? Or does it imply a small/little functional impact, which cannot be determined by appearance alone?
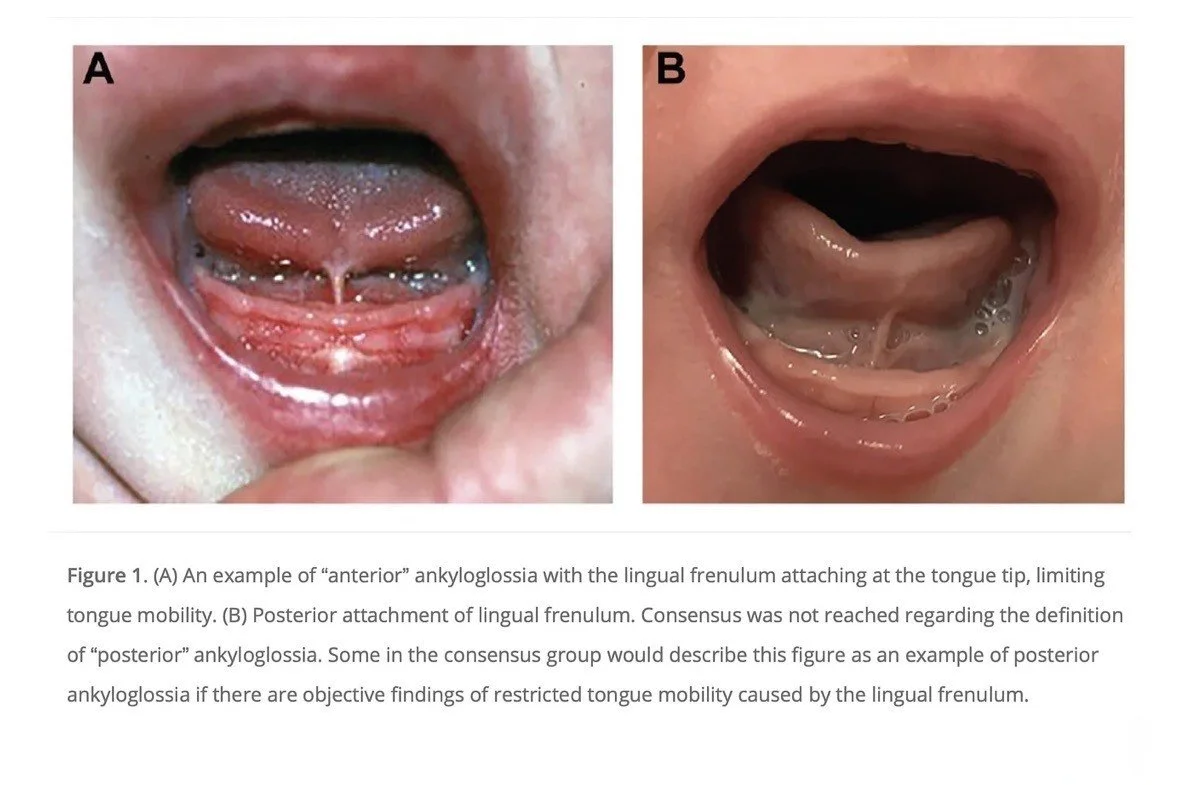
From Messner AH, Walsh J, Rosenfeld RM, et al. “Clinical Consensus Statement: Ankyloglossia in Children.”
Otolaryngology–Head and Neck Surgery. 2020;162(5):597–611.
If your baby or child is experiencing challenges, it’s worth seeking a second opinion from a clinician who evaluates tongue ties based on function and appearance, not just appearance alone. Ensure the provider you see has as special interest and plenty of experience in oral ties.
When I assess a child, I am less interested in whether the frenulum looks big or small and more interested in how well the tongue can actually move and there are validated tools that help us measure this.
How the tongue should move
Key points:
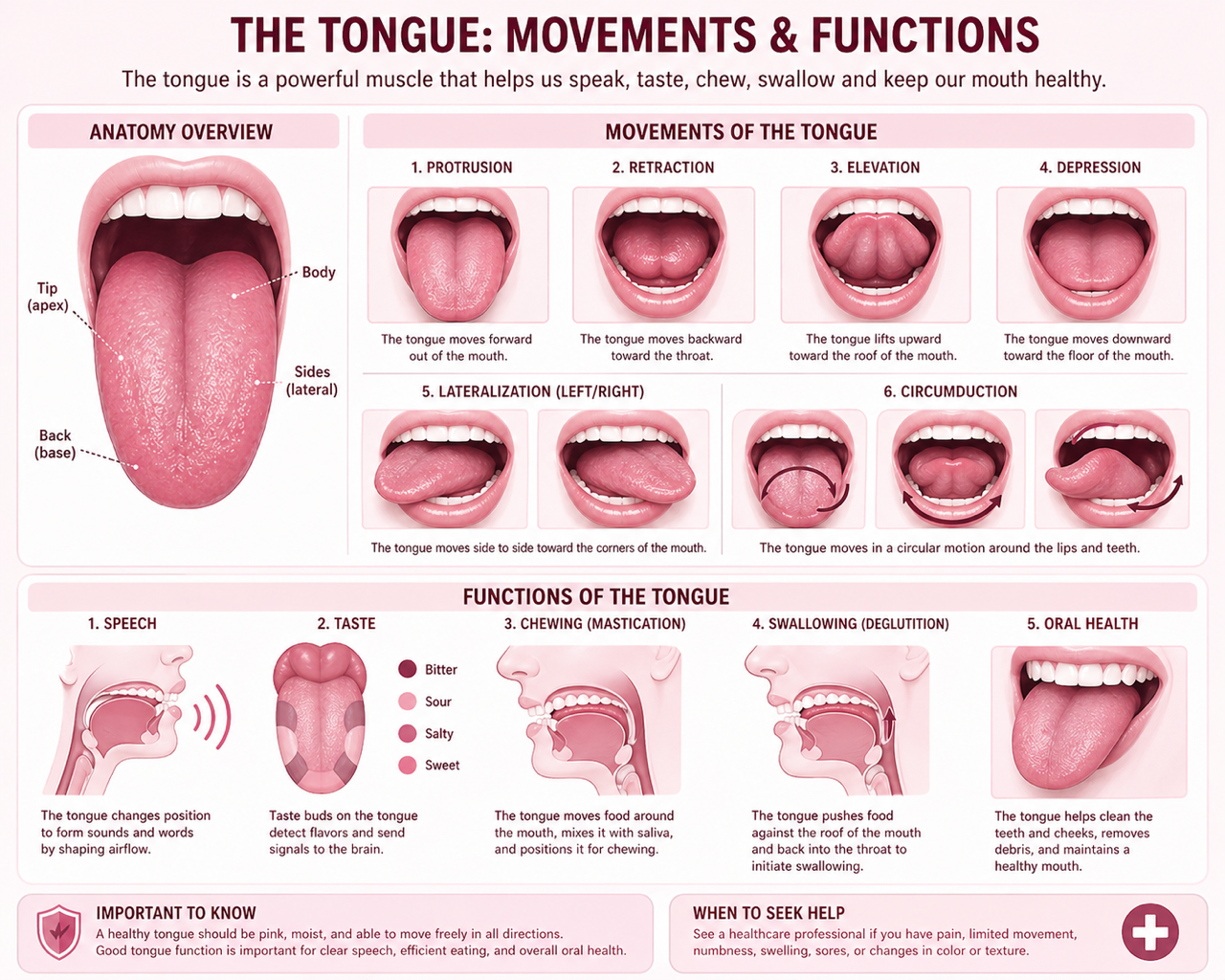
The tongue needs a full range of motion: up to the palate, down, side to side, and forwards past the lower gum line to feed, swallow, clear the mouth, and develop speech.
Normal function includes creating and maintaining suction at the breast, coordinated peristaltic wave along the tongue, lifting to the palate during swallowing, and resting lightly on the palate between swallows.
“Imagine trying to talk, swallow and keep your teeth clean while your tongue is tethered with a tight band of string-like tissue – even if that string is short and hard to see, your tongue still cannot move freely.”
What a tongue tie is and how it can restrict movement
A tongue tie (ankyloglossia) is where the band of tissue under the tongue (the lingual frenulum) is tighter, shorter or placed in a way that restricts tongue movement. Some frenula are very obvious - attaching right near the tip of the tongue - but others are more subtle, sitting further back or hidden under the surface. Either way, the important question is: does this frenulum limit how the tongue moves and function in everyday life?
A restrictive tongue tie can lead to:
Breastfeeding difficulties - shallow latch, sliding or “chomping” at the breast, prolonged or very frequent feeds, clicking, leaking milk, poor milk transfer, nipple pain and damage, and sometimes slow weight gain or failure to thrive.
Bottle feeding issues - clicking, leaking, prolonged feeds, coughing or spluttering, or a baby who tires quickly at the bottle.
Older infant and child feeding problems - difficulty moving food around the mouth, gagging on lumps, pocketing food in the cheeks, messy eating, dribbling, or difficulty licking an ice cream or clearing food off the teeth.
Speech concerns - trouble producing sounds that need good tongue elevation and precision (t, d, l, n, r, s, z, th), or a child who works very hard to make these sounds.
Other oral and airway issues - difficulty keeping the mouth clean, altered jaw and dental development, open‑mouth posture, snoring or restless sleep in some children.
So while a frenulum might look “small”, if it is significantly limiting elevation, protrusion or side‑to‑side movement, it can still have a big impact on function for that particular child.
“Mild” on paper, significant in real life
This is where many families get stuck.
They are told the tongue tie is “mild”, “little”, “small”, or “not that bad”, so it must be unrelated to the problems they are seeing. However, research and clinical experience both tell a more nuanced story, and a tie can be graded as “mild” using one anatomical scale, yet still meaningfully limit how the tongue can move. Studies have shown that when a baby has clear functional breastfeeding problems and a restrictive frenulum, even if the tie looks small, releasing it can make a real difference for some families.
Beyond infancy
A scoping review of tongue tie release in older children and adults has shown significant improvements in tongue mobility, speech, oral comfort and in some cases sleep‑related symptoms after surgery. Again, the key predictor of benefit was not how dramatic the frenulum looked in a photo, but how much it limited function before treatment and how much movement improved afterwards.
All of this supports what many parents already sense: if a tongue tie is causing obvious problems, it is not “just a little tie” for their child.
When a “little tie” is not a little problem
So when should you start questioning the “it’s just a little tie” message?
In babies, it is reasonable to seek a more detailed assessment if your baby has these symptoms despite good lactation and positioning support:
Painful breastfeeding.
Ongoing shallow latch, clicking, slipping off the breast or prolonged, frequent feeds.
Poor weight gain or concerns about milk transfer.
Reflux‑like behaviour, excessive gassiness or very unsettled feeding.
These issues can have multiple causes, but a functionally significant tongue tie is one possibility that deserves careful consideration, especially when you have already tried standard breastfeeding support.
In older infants and children, you might want a second opinion if your child has:
Persistent gagging, choking or difficulty advancing textures.
Very messy eating, food trapped in the cheeks, or trouble clearing food from the teeth.
Speech that is unclear or difficult for others to understand, particularly if certain sounds are hard despite therapy.
Open‑mouth posture, mouth breathing, snoring or very restless sleep.
Ongoing oral hygiene problems, bad breath or dental issues that relate to tongue position and movement.
Not every child with a visible frenulum will have these problems, and not every difficulty in these areas is caused by a tongue tie. However, if several of these signs are present and you have been told it is “just a little tie”, it is absolutely appropriate to ask whether that assessment looked carefully at function, not only at appearance.
Why a second opinion matters
There is no single, universally accepted guideline that fits every tongue tie scenario, and even experts disagree at times. That is why a thorough, functional assessment from someone experienced in this area is so important.
A good evaluation should include:
A detailed history of feeding, growth, speech, sleep and any other symptoms.
Careful examination of tongue movement - elevation, protrusion, side‑to‑side motion and how the tongue shapes and rests in the mouth.
Observation of breastfeeding or feeding where possible.
If a frenotomy or frenuloplasty is recommended, it should be part of a team plan that also includes:
Pre - and post‑procedure feeding support.
Oral motor or myofunctional therapy where appropriate.
Follow‑up to monitor healing, function and progress.
As a tongue tie doctor on the Gold Coast, I often meet families who feel dismissed because they were told their baby or child only has a “little tie” while problems continued. Your concerns and your lived experience at home are important data points, and they deserve to be taken seriously alongside the examination findings.
Tongue tie doctor Gold Coast: how I can help
If you are on the Gold Coast and worried that a “mild” tongue tie may be contributing to your baby’s or child’s difficulties, I offer:
Comprehensive oral tie assessment focused on appearance and function.
Infant tongue tie procedures (where appropriate), performed with a focus on comfort and safety.
Close collaboration with local lactation consultants, speech pathologists, physiotherapists, osteopaths, chiropractors and oromyofacial therapists.
Sometimes, after a detailed assessment, we may decide that watching and supporting is the best plan, other times, we may agree that a release offers a good chance of improving feeding, or comfort and preventing future issues. The goal is always the same: to make sure that, if the tie is not so little in its impact, it is not ignored.
If you have seen a lactation consultant and a bodyworker and are still having challenges and would like to discuss your situation further, you can book an appointment at my clinic on the Gold Coast to explore whether your child’s tongue tie is truly “little” - or whether it is time for a closer look.
References (for further reading)
Ballard JL, Auer CE, Khoury JC. Ankyloglossia: assessment, incidence, and effect of frenuloplasty on the breastfeeding dyad. Pediatrics. 2002;110(5):e63.
Bruney TL, Scime NV, Madubueze A, et al. Systematic review of the evidence for resolution of common breastfeeding problems-ankyloglossia (tongue tie). Acta Paediatrica. 2022;111(5):940-947. doi:10.1111/apa.16289
Coryllos E, Genna CW, Salloum AC. Congenital tongue-tie and its impact on breastfeeding. AAP News. 2004;25(7):1‑6.
Daggumati S, Cohn JE, Brennan MJ, Evarts M, McKinnon BJ, Terk AR. Speech and language outcomes in patients with ankyloglossia undergoing frenulectomy: a retrospective pilot study. OTO Open. 2019;3(1):2473974X19826943. doi:10.1177/2473974X19826943.
Francis DO, Krishnaswami S, McPheeters M. Treatment of ankyloglossia and breastfeeding outcomes: a systematic review. Pediatrics. 2015;135(6):e1458-e1466. doi:10.1542/peds.2015-0658.
Ghaheri BA, Cole M, Fausel SC, Chuop M, Mace JC. Breastfeeding improvement following tongue‐tie and lip‐tie release: a prospective cohort study. Laryngoscope. 2017;127(5):1217‑23.
Hatami A, Dreyer CW, Meade MJ, Kaur S. Effectiveness of tongue-tie assessment tools in diagnosing and fulfilling lingual frenectomy criteria: a systematic review. Australian Dental Journal. 2022;67(3):212-219. doi:10.1111/adj.12921.
Messner AH, Walsh J, Rosenfeld, RM, Schwartz SR, Ishman SL, Baldassari C, Godoy J. Clinical consensus statement: Ankyloglossia in children. Otolaryngology–Head and Neck Surgery. 2022; 162(5), 597–611.
Miranda BH, Milroy CJ. A quick snip - a study of the impact of outpatient tongue tie release on neonatal growth and breastfeeding. Journal of Plastic, Reconstructive & Aesthetic Surgery. 2010;63(9):e683‑5.
Necus E, Claessen M, Hennessey N, Smart S. Assessment of tongue structure and function in infants for the diagnosis of ankyloglossia: A systematic xreview. International Journal of Pediatric Otorhinolaryngoly. 2025 Sep;196:112485. doi:10.1016/j.ijporl.2025.112485.
Power RF, Murphy JFA. Tongue‐tie and frenotomy in infants with breastfeeding difficulties: achieving a balance. Archives of Disease in Childhood. 2015;100(5):489‑94.
Shekher R, Lin L, Zhang R, Hoppe IC, Taylor JA, Bartlett SP, Swanson JW. How to treat a tongue‑tie: an evidence‑based algorithm of care. Plastic Reconstructive Surgery - Global Open. 2021 Jan 25;9(1):e3336. doi: 10.1097/GOX.0000000000003336.
Suter VGA, Bornstein MM. Ankyloglossia: facts and myths in diagnosis and treatment. Journal of Periodontology. 2009;80(8):1204‑19.
Webb AN, Hao W, Hong P. The effect of tongue‐tie division on breastfeeding and speech articulation: a systematic review. International Journal of Pediatric Otorhinolaryngoly. 2013;77(5):635‑46.